


Contact Admission
International Collaboration




Can Cardiovascular Risk Assessment Be Improved in the 21st Century?
Thomas A. Gaziano, MD, MSc1; J. Michael Gaziano, MD, MPH2
JAMA. Published online May 13, 2024. doi:10.1001/jama.2024.7644
Cardiovascular risk assessment has become an essential part of preventive strategies designed to target risk factor interventions and has contributed to dramatic reductions in cardiovascular disease mortality during the past 60 years in the US and other countries. Beginning in the 1960s, investigators from the Framingham Heart study1,2 identified key physiological, behavioral, and biochemical risk factors for atherosclerotic cardiovascular disease and were the first to develop multivariable risk equations using major risk factors to predict first-time fatal and nonfatal myocardial infarction and later atherosclerotic cardiovascular disease events during a period of up to 12 years.3 These risk equations are able to explain about 70% to 80% of the variability of cardiovascular risk in the populations in which they were derived.4 The generalizability of these early tools has been enhanced by using large, diverse, pooled cohorts in the US (American Heart Association/American College of Cardiology Pooled Cohort Risk Equation),5 Europe (European Society of Cardiology Systematic Coronary Risk Evaluation 2 [SCORE2]),6 and elsewhere. Since their development, many attempts to improve the models have been pursued, yet the basic models have stood the test of time.
Other Case Report
- Challenges in Clinical Electrocardiography – A Mysterious Case of ST Elevation ( 10:29 - 15/09/2025 )
- New Secrets About Psoriatic Arthritis: Is Combination Therapy as Safe as You Think? ( 14:33 - 06/09/2025 )
- Mitrofanoff procedure: more 40 years later. ( 07:36 - 28/03/2025 )
- Telehealth vs In-Person Early Palliative Care for Patients With Advanced Lung Cancer ( 09:26 - 12/10/2024 )
- ST-Segment Elevation in a Woman With Out-of-Hospital Cardiac Arrest ( 08:35 - 24/09/2024 )
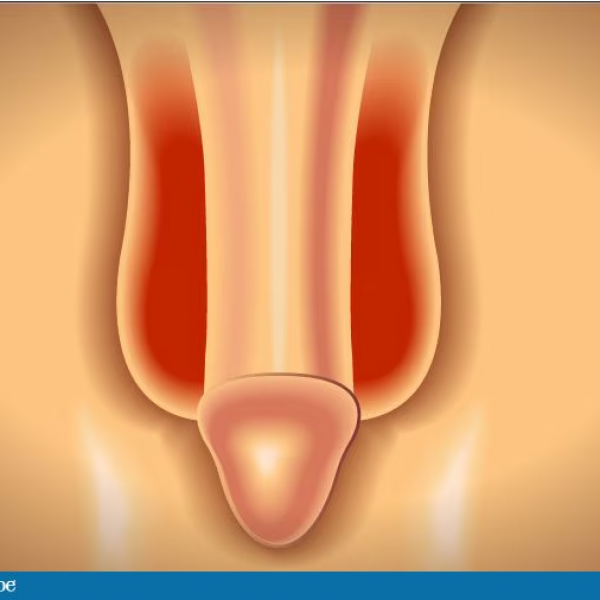
- Scrotal Rash for Months ( 11:07 - 31/05/2024 )
- Lower Gastrointestinal Hemorrhage ( 16:15 - 16/05/2024 )
- Approach to Obesity Treatment in Primary Care ( 14:04 - 20/03/2024 )
- Fever, Rash, and Shortness of Breath in a 69-Year-Old ( 09:20 - 04/03/2024 )
PHAN CHAU TRINHUNIVERSITY
- 09 Nguyen Gia Thieu street,
Dien Ban Dong ward,
Da Nang city
Phan Chau TrinhUniversity’s Hospital
- 09 Nguyen Gia Thieu street,
Dien Ban Dong ward,
Da Nang city







